
Download the PDF.
Leaders recognize that reversing this dynamic requires new sources of margin-accretive revenue growth, yet existing structures make those efforts hard to pursue. Growth initiatives often collide with near-term financial targets and are dismissed as taking too long to pay off. As a result, hospital leaders default to cost reduction, believing it is the lever they can control most reliably. Our latest industry research shows that while executives prioritize revenue growth, cost containment remains their primary focus.
But leaders can make growth a consistent driver of margin—right alongside cost control. By adopting a product mindset and redesigning operations around patient choice, organizations can differentiate how care is delivered and improve performance to generate meaningful margin relief. When hospital systems make explicit choices about where to focus growth and reinforce those choices through changes in how the organization works, margin improvements can be sustained and built upon over time.
This article examines how healthcare providers can make growth disciplined by viewing it through three connected lenses: the products they deliver, the portfolio of opportunities they pursue, and the operating model that enables execution. Drawing on work with clients and broader industry insights, we show how these lenses help build growth as a core capability that supports long-term financial sustainability.
Develop a product mindset for patient care.
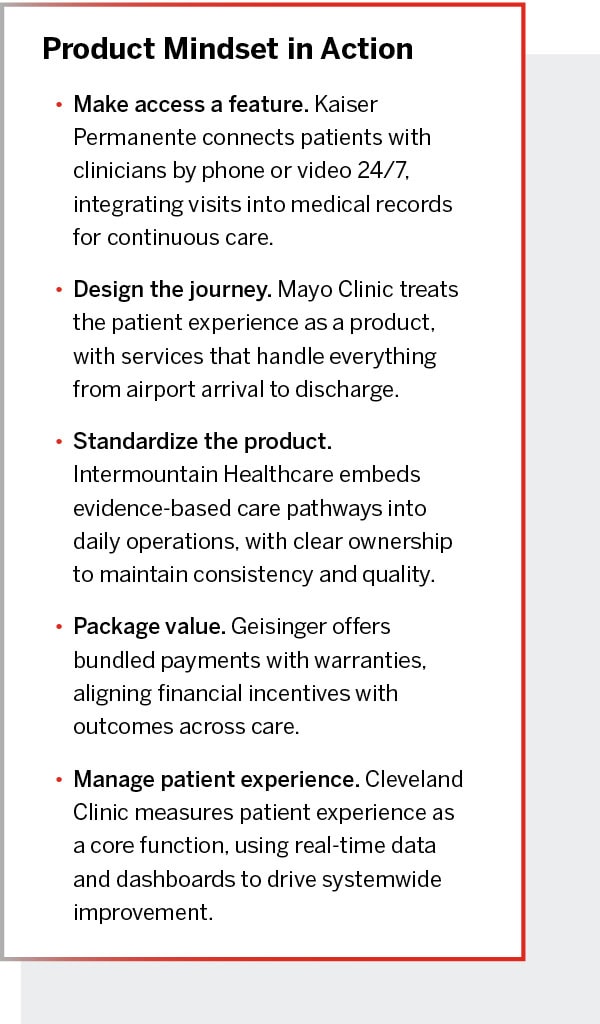 Every hospital system is competing to grow its highest-margin programs, and financial performance increasingly depends on elective procedures and patient retention. In this environment, consumer choice and loyalty shape the bottom line. Growth depends on understanding what patients are trying to accomplish and designing care experiences around that journey.
Every hospital system is competing to grow its highest-margin programs, and financial performance increasingly depends on elective procedures and patient retention. In this environment, consumer choice and loyalty shape the bottom line. Growth depends on understanding what patients are trying to accomplish and designing care experiences around that journey.
Yet many organizations struggle to do that. Healthcare has lagged in adopting a product mindset in part because integrated systems were built to be everything to everyone. That legacy has produced complex, inefficient models. Many still make decisions about services at the individual hospital level, with each site determining what it will offer. That approach results in high-cost programs being replicated across facilities, creating internal competition for patients even when the economics or volumes aren’t viable.
Developing a product mindset changes the approach to service planning. Instead of starting with individual hospital verticals, leaders look across service lines at the market or regional level and decide what services should be delivered where. That shift clarifies which services matter most for growth and sets clear expectations for how those services should perform. Over time, the care delivery portfolio becomes the result of deliberate choices rather than an outcome shaped by legacy organizational structures and silos.
Ascension Health in Texas demonstrated this by focusing on a specific challenge: keeping cancer treatment on track for patients with underlying cardiovascular risk. Leaders saw that outcomes depended heavily on where patients began their journey. Some received early cardiac screening and monitoring that allowed therapy to continue uninterrupted. Others encountered delays or inconsistent evaluation, increasing the risk that heart complications would disrupt care. Rather than treating cardio-oncology as a set of services offered locally, Ascension redesigned it as a single, systemwide pathway that followed patients from diagnosis through treatment, reorganizing delivery across eight hospitals and ten outpatient sites.
 That redesign required the organization to take ownership of how the service performed end to end. Clinical protocols defined when and how cardiac risk was assessed, and oversight was centralized to manage delivery across locations. One early execution step focused on diagnostic consistency: echocardiography technologists were retrained so imaging was performed and reported the same way at every site. As demand grew, a live registry tracked patient access and flow across the system, allowing leaders to identify delays and capacity constraints. With fewer disruptions to care and more reliable access, service volume increased sixfold while patient experience improved.
That redesign required the organization to take ownership of how the service performed end to end. Clinical protocols defined when and how cardiac risk was assessed, and oversight was centralized to manage delivery across locations. One early execution step focused on diagnostic consistency: echocardiography technologists were retrained so imaging was performed and reported the same way at every site. As demand grew, a live registry tracked patient access and flow across the system, allowing leaders to identify delays and capacity constraints. With fewer disruptions to care and more reliable access, service volume increased sixfold while patient experience improved.
Services perform best when organizations design them around how patients actually experience care and take ownership for the results those experiences produce. Leaders focus on who they serve and what patients are trying to accomplish, then shape delivery models to meet those needs in ways that create real differentiation. When care is accessible and works reliably, demand grows, patient preference strengthens, and conversations with payers shift. Over time, tracking engagement and adoption alongside quality and cost allows providers to refine offerings and support growth with greater economic discipline.
Design an operating model fit for growth.
When growth stalls, the issue is usually structural. Even when providers define services at the system level to better reflect patient needs, existing operating models—built for cost control, quality, and reliability—aren’t designed to manage those services consistently across sites or adapt well to shifting demand. Making that shift work requires changes in how the organization operates: clearing barriers, setting new priorities, and enabling teams to act. As those changes take hold, growth becomes easier to sustain.
We advised a regional health system that confronted this issue when its operating model became too fragmented to support its ambitious growth agenda. Each service line pursued its own priorities, and regional leaders often made decisions in isolation. Individual hospitals competed with service line leaders for resources that should have been deployed toward shared goals, particularly efforts to expand in ambulatory and complex care delivery. Misaligned incentives and long-standing tensions between different operating units made it impossible to meet growth and performance targets, or to allocate resources across key business units.
The system addressed this by making service lines the organizing unit for strategic planning and performance management, not just clinical oversight. It clarified accountability for results, such as volume growth, across the network. For example, the cardiovascular service line leader became responsible for both quality and growth at every site, not just one hospital. At the same time, regional operations were reorganized into a hub-and-spoke model, with flagship sites anchoring high-acuity care while community hospitals and ambulatory centers extended access.
That shift also changed how clinical and operational leadership worked together. Service lines assumed broader responsibility for performance across sites, with clearer authority to make decisions that previously required negotiation across multiple roles. This simplified the leadership structure by reducing duplicated oversight between service lines and central functions while clarifying who was responsible for outcomes. As a result, the organization could act more decisively when priorities competed.
Those changes were reinforced through new governance and planning processes that linked decisions about capital, staffing, and referrals to overall growth priorities. Leadership reviewed performance and investment choices through a unified, systemwide view connecting market strategy with operational planning. This discipline helped translate strategic intent into day-to-day operating decisions. Over time, it created more consistency across regions and positioned the organization to focus resources on expanding complex care.
What became clear was that execution challenges were rarely about tools or policies alone. Culture shaped whether leaders were willing to disrupt old routines and whether physicians trusted the direction of change. The operating model redesign worked because it tackled those cultural undercurrents alongside the technical fixes.
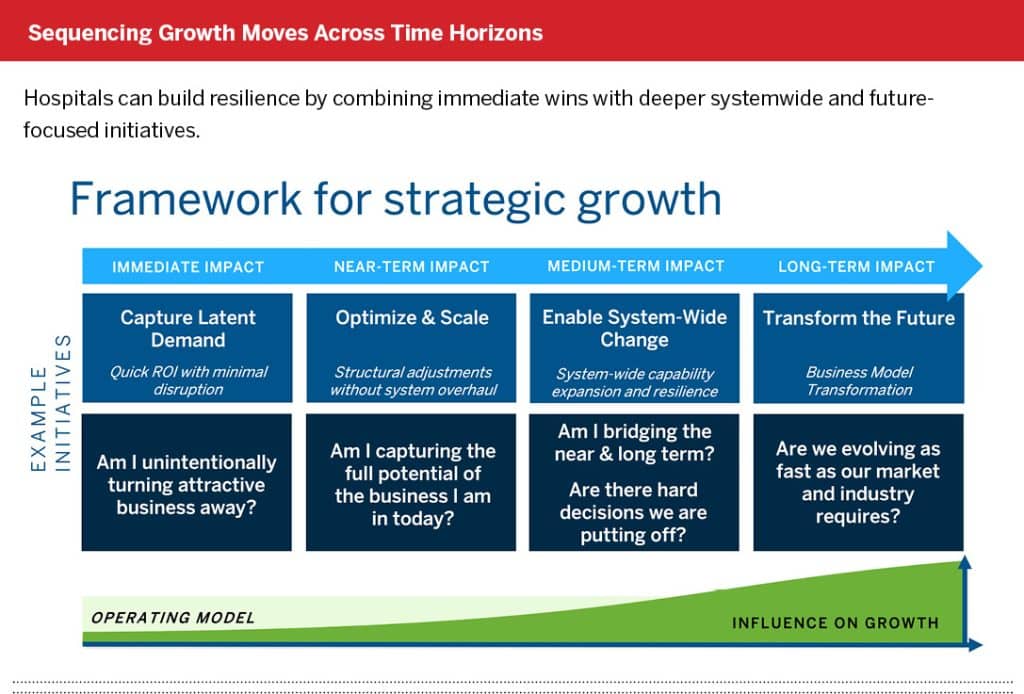
Build a portfolio for growth and resilience.
Growth isn’t a single initiative—it’s a discipline. Effective strategies unfold across multiple time horizons, combining quick wins with longer-term investments that prepare care providers for market shifts.
That’s especially important for cash-strapped systems. Growth is often dismissed as a future luxury, but some actions can deliver near-term margin impact. Others build the flexibility to respond to emerging challenges instead of being blindsided by them. This ability to keep moving forward—even in uncertainty—is what sets resilient organizations apart.
A regional health system we advised reassessed its growth agenda after recognizing that incremental improvements would not close its margin gap. Cost actions had stabilized performance, but growth stalled as leadership attention and investment remained tied up in small, disconnected efforts across the organization. Rather than launching another wave of initiatives, it concentrated on a limited number of services where stronger performance would materially affect margins and competitive position.
The work started by removing constraints that limited performance in those services, beginning with access and utilization. “Tiger teams” examined referral patterns and care pathways and found that demand was leaving or getting stuck behind internal bottlenecks. In cardiovascular care, for instance, shortages of specialized surgical staff limited throughput despite strong demand. It adjusted staffing models and scheduling practices to relieve those constraints, allowing existing capacity to support higher volumes without new capital investment.
As performance improved, leadership reconsidered how services were distributed across hospitals. Instead of maintaining the same high-cost capabilities everywhere, specialized services were consolidated so they could operate at scale. Programs such as bariatrics and other complex surgical services were concentrated at a single, high-quality hub, while pre- and post-care shifted closer to patients through neighborhood clinics and home-based settings. Operating room policies were changed to reduce delays for complex procedures, and appropriate cases were shifted into ambulatory settings.
With capacity freed and results improving, the organization made further changes to how care was organized across the network. Services were reassigned among nearby campuses so each site focused on a narrower role, including redesigning one campus around behavioral health while shifting medical and surgical volumes to others. These moves linked near-term gains to longer-term changes in the care model, allowing the provider to invest in growth without stepping away from its community commitments.
________
Hospital systems can’t close margin gaps through cost control alone. Disciplined growth begins with a shared understanding of patients and communities that enables providers to design offerings that truly stand apart. When those efforts are advanced through a portfolio that balances immediate performance with longer-term transformation, and are supported by an operating model built to sustain them, growth becomes a lasting capability that strengthens both the organization and the care it provides.
About the Authors
KC Loder is a Managing Director at Innosight. kloder@innosight.com
Andy Waldeck is the Global Managing Partner of Innosight and co-leader of the healthcare practice. awaldeck@innosight.com
Endnotes
- Liu, Yan, “A novel cardio-oncology service line model in optimizing care access, quality and equity for large, multi-hospital health systems,” National Library of Medicine, 2023.